


While Clallam and Jefferson counties desperately need more mental health services, Jamestown Salish Seasons’ grand opening next month and patient admissions starting in September come with a major caveat: This tribally operated facility is positioned to generate substantial revenue from taxpayers through special billing advantages that let it charge and collect far more per patient encounter than non-tribal providers. What’s billed as a bold community service also represents a lucrative business model for the Jamestown Corporation.
A Needed Service...
According to the Sequim Gazette, Jamestown Salish Seasons will begin accepting patients on September 28 following its August 26 grand opening. The $31.25 million facility will provide voluntary psychiatric evaluation and treatment twenty-four hours a day in a secure 16-bed facility designed for patients experiencing severe depression, suicidal ideation, psychosis, and other acute mental health crises.

There is little debate that the Olympic Peninsula needs more mental health resources. Families have long struggled to find voluntary treatment before a crisis reaches the point of involuntary commitment. If Salish Seasons succeeds in filling that gap, it will undoubtedly benefit many people.
But as with nearly every large healthcare expansion by the Jamestown Corporation, there’s another side of the story.
“Local” Patients...and Patients From Across Washington
The Gazette reports that patients will come from Clallam County, Jefferson County, and citizens of Washington’s federally recognized tribes.
That means the facility isn’t simply serving the North Olympic Peninsula. Depending on capacity, it has the potential to serve tribal citizens from throughout the state.

What Was the State Concerned About?
Executive Director Matt McKnight told the Sequim Gazette the opening was delayed because of negotiations with state regulators.
According to McKnight, the tribe was doing something “bold and different,” making it difficult for regulators to “wrap their mind around” the new model. He also acknowledged that negotiations over reimbursement rates with Washington’s managed care organizations contributed to the delay.
That’s an explanation—but not much of one. What exactly was the state uncomfortable with? Was it licensing? Patient care standards? Payment rates? Operational policies?
Those details matter, yet they remain unanswered.

Thirty New Employees—From Where?
The tribe also plans to hire approximately thirty new employees, many in entry-level positions including recovery specialists, treatment coordinators, cooks, custodians, and maintenance staff.
That’s good news for job seekers. It’s potentially less welcome for existing employers.
Businesses throughout Clallam County have spent the past several years struggling to hire and retain workers. Every major employer that expands its workforce pulls from the same limited labor pool. The obvious question is how many local businesses will lose experienced employees as Jamestown continues expanding its healthcare empire.

A Different Way of Getting Paid
Perhaps the most interesting part of the Gazette’s coverage wasn’t about the building at all. McKnight explained that voluntary psychiatric treatment is more difficult to finance because insurance companies don’t always guarantee payment the way they do for involuntary commitments. He said Jamestown ultimately negotiated reimbursement rates based on the actual operating costs of the sixteen-bed facility.
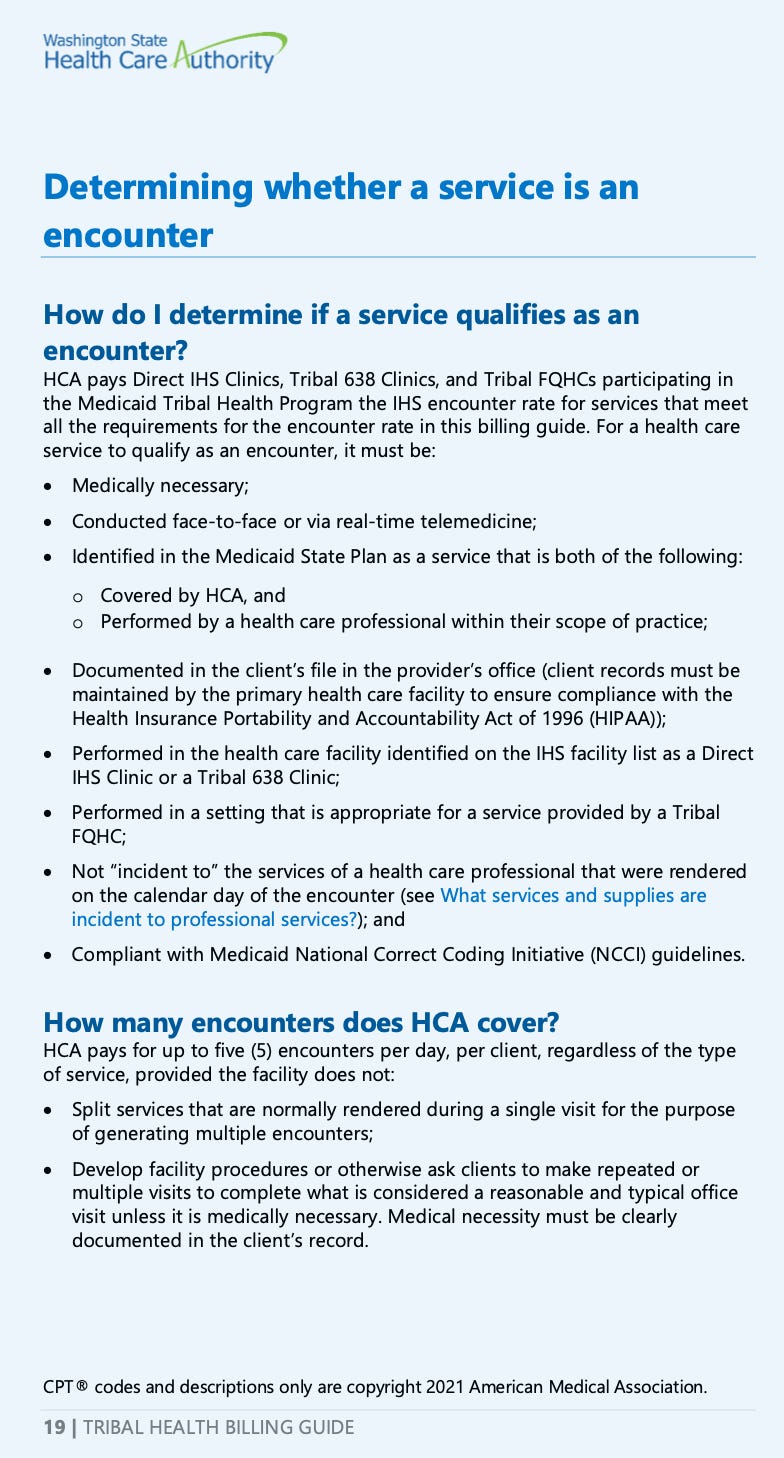
That statement deserves far more attention than it received. Most people have never heard of Indian Health Service encounter rates. They probably should.
Unlike traditional healthcare providers, eligible tribal clinics can receive federally established all-inclusive reimbursement rates for qualifying patient encounters. Those rates continue to climb. The federal outpatient encounter rate for Lower 48 tribal facilities increased to approximately $826 per qualifying encounter in 2026, and Washington’s Tribal Health Billing Guide allows multiple qualifying encounters during a single day under certain circumstances when different services are provided.
Medications and other services may also be billed separately when allowed under state and federal rules.
That’s not a loophole. It’s federal policy. But it is a payment structure unavailable to most community hospitals, physician offices, and independent healthcare providers.
Why the Tribe Keeps Expanding Healthcare
For years, the Jamestown Tribe has steadily expanded beyond its casino, adding medical clinics, behavioral health, medication-assisted treatment, pharmacies, dental services, and now a psychiatric hospital.
Viewed individually, each project looks like another community investment.
Viewed together, they represent something much larger: a healthcare system built around reimbursement rules that are substantially different from those available to non-tribal providers. Those rules create powerful incentives to continue expanding services because each qualifying encounter generates additional revenue.
If a single Medicaid patient visits Jamestown Family Health, the Jamestown Dental Clinic, the MAT clinic, the pharmacy, and later has a qualifying telehealth appointment, the reimbursement from those encounters could exceed $4,000 in a single day, depending on eligibility and billing rules.
A Different Recovery Model
The debate becomes even more interesting when treatment outcomes are compared.
The Salvation Army’s Adult Rehabilitation Program in Seattle provides up to fourteen months of residential treatment, work therapy, job placement assistance, and transitional housing without relying on Medicaid encounter-rate billing. According to the organization, about 38 percent of participants successfully complete the program, and among graduates who remain connected for two years, approximately 86 percent maintain sobriety.

Jamestown’s Medication-Assisted Treatment program has reported strong patient retention, but retention is not the same thing as recovery. Taxpayers should be asking harder questions.
How many people return to work?
How many become financially independent?
How many remain drug-free years after treatment?
Those are the outcomes that matter. Yet the answers remain largely out of public view, shielded behind the sovereignty of a tribal government receiving millions in taxpayer-funded reimbursements.
A Call For Transparency
None of this is an argument against providing mental health care. Salish Seasons may become an important resource for our community and save lives in the process.
But taxpayers deserve transparency about more than the opening date and ribbon cutting. They deserve to understand why tribal healthcare facilities are reimbursed differently, how much those differences are worth, and whether the incentives encourage long-term recovery—or simply long-term billing.
That’s a conversation worth having. And it’s one that too few people are willing to start.
Today’s Tidbit: $25.7 Million Housing Fund — Who Gets to Apply?
Washington taxpayers are helping fund the state’s Housing Trust Fund, but this latest $25.7 million set-aside is only available to one group: federally recognized tribes with land in Washington and their tribally controlled housing entities.
According to the Washington State Department of Commerce, eligibility is limited to federally recognized tribes or Tribally Designated Housing Entities (TDHEs) operating under tribal control.
The question for taxpayers: When public dollars are collected statewide, should programs like this be open to all eligible housing providers, or reserved exclusively for sovereign tribal governments?
